Closing in
0
...
Menu
Search
LATEST
POPULAR
AIRCRAFT FOR SALE
SECTIONS
Business Aviation
Defense
Aerospace & Air Transport
FutureFlight
Rotorcraft
General Aviation
SUSTAINABILITY & ENVIRONMENT
CHANNELS
Aircraft
Maintenance
Avionics
Charter & Fractional
Safety
All Categories
News Archive
Newsletter Archive
MORE
AIN FBO Survey
Airshows & Conventions
Aviation Events
Compliance Countdown
Expert Opinion
In-Depth Reports
Leeham News & Analysis
Print Archives
Videos
Webinars
Whitepapers
ABOUT
About AIN
Our Writers
History
Advertise
Contact Us
Subscribe
LATEST
POPULAR
AIRCRAFT FOR SALE
SECTIONS
ABOUT
Search
Subscribe
Search
Accidents
Business Aircraft Accident Reports: March 2025
Preliminary and final accident reports, March 2025
Share
Post
Share
Print
Copy
Email
By
David Jack Kenny
• Contributor - Safety
March 3, 2025
More In Accidents
Grand Caravan Crash at Heritage Site in Peru Kills 13
Aerodiana confirms it operated the sightseeing flight over the Nazca Lines archaeological site
Accidents
Two Killed in Greek Helicopter Midair Collision
A pair of Bell 412STs collided while fighting fires near Athens
Accidents
Business Aircraft Accident Reports: August 2026
Preliminary and final accident reports, August 2026
Accidents
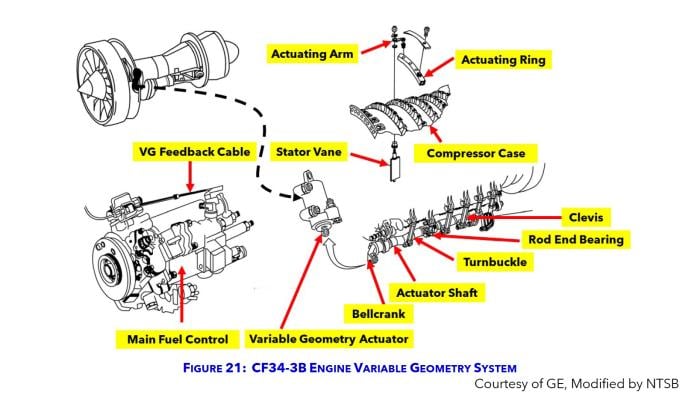
Comment Period Closes on GE CF34 Engine Corrosion AD
FAA action would require more inspections for affected turbines
Accidents
Uncoordinated Flight Eyed in TBM 850 Manitoba Flameout
One of four aboard taken to hospital with minor injuries
Accidents
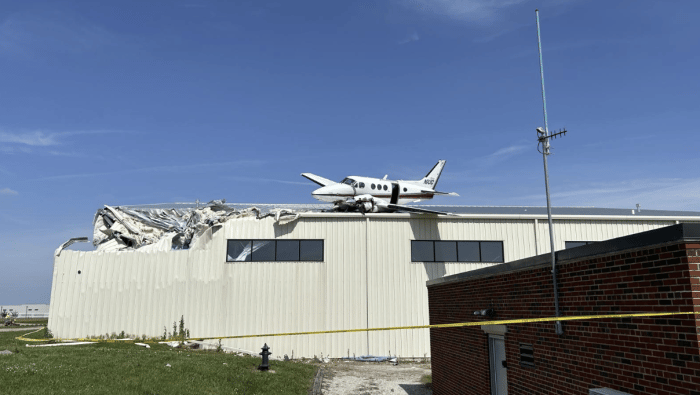
Fuel Exhaustion Left King Air Crew Out of Time, Altitude
AFM prohibits takeoff with fuel in yellow caution band; instructor failed to supervise airspeed in pattern
Accidents
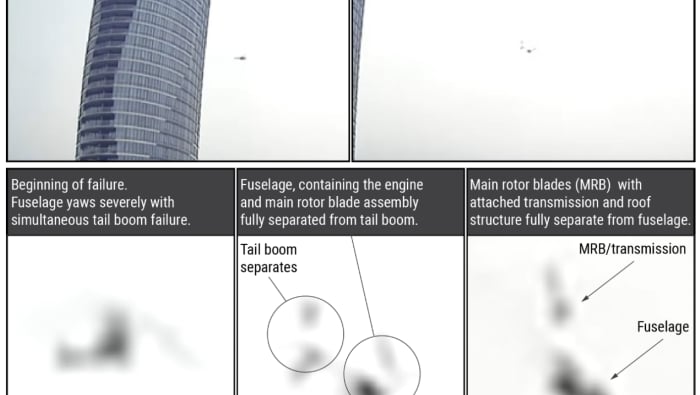
NTSB Eyes Goose Strike in Fatal Hudson Helicopter Crash
Smithsonian analysis found goose remains on rotor blades
Accidents
Fuel System Components Eyed in NetJets Citation Crash
NTSB found damaged starter generator and fractured fuel assembly
Accidents